
Case #14
-
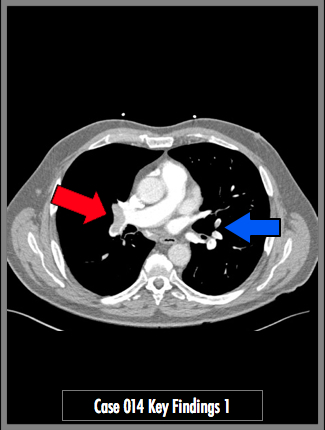
History: Chest Pain, Elevated D-dimer, Shortness of Breath
© 2012 Must See Radiology
History: Chest Pain, Elevated D-dimer, Shortness of Breath
© 2012 Must See Radiology


Contrast enhanced CT of the chest in the axial plane (1) and coronal maximal intensity projection (MIP) (2)


Contrast refluxing into the IVC and into the hepatic veins is CT evidence for elevated right heart pressures. It is an indirect sign of tricuspid valve insufficiency. Elevated right heart pressures can be seen in pulmonary embolism. When PE is identified on CT, another measurement that can help with severity of disease is the RV/LV ratio, i.e. the width of the right ventricle related to the left ventricle. The normal ratio of RV width to LV width should be no more than 0.9. Right heart strain is suspected when the RV/LV ratio is greater than 1. See Radiographics Article in References for measurement info. See another PE case for an example of massive PE with extensive right heart strain.
© 2012 Must See Radiology
Acute Pulmonary Embolism
Findings show a bilateral acute pulmonary embolism. The right side show thrombus extending into the branches of the middle and lower lobes. It appears to "saddle" the two branches, however, this is NOT a true saddle pulmonary embolism. A true "Saddle PE" requires the thrombus to extend from the left to the right pulmonary arteries. An example of this is presented in another case.
This patient presented with a V/Q scan (Case 13) which demonstrated a large mismatched perfusion defect in the the lower right lung.
When evaluating pulmonary embolism on CT, always check for the adequacy of opacification in the pulmonary arteries. The theoretic minimum pulmonary artery enhancement HU for detection of acute and chronic pulmonary emboli are 93 and 211, respectively. The greater pulmonary artery enhancement, the greater conspicuity of emboli. Ideal studies will have enhancement HU > 300. When the HU is < 200, pulmonary embolism may not be detected and this should be noted in the report. Repeating the contrast bolus and scan may be helpful, in the appropriate clinical setting.
Additional Information:
Sostman, HD. "Acute Pulmonary Embolism: Sens and Spec of Ven-Perf Scintigraphy in PIOPED II Study." Radiology Jan 2008, 246:941-946.
Stein, PD. "Contrast enhanced multidetector spiral CT of the chest and lower extremities in the suspected acute pulmonary embolism: results of the PIOPED II." NEJM 2006, 354:2317-2327.
The PIOPED Investigators. "Value of the ventilation/perfusion scan in acute pulmonary embolism: results of the Pulmonary Embolism Diagonsis(PIOPED)". JAMA 1990, 263: 2753-2759.
Wittram C. "How I do it: CT pulmonary angiography." AJR 2007, 188: 1255-1261.
© 2012 Must See Radiology
Not available at this time.
Rating not available at this time.
Any feedback regarding this case can be emailed to Tony@mustseeradiology.com
Thank you for trying Must See Radiology!
© 2012 Must See Radiology