Key Findings
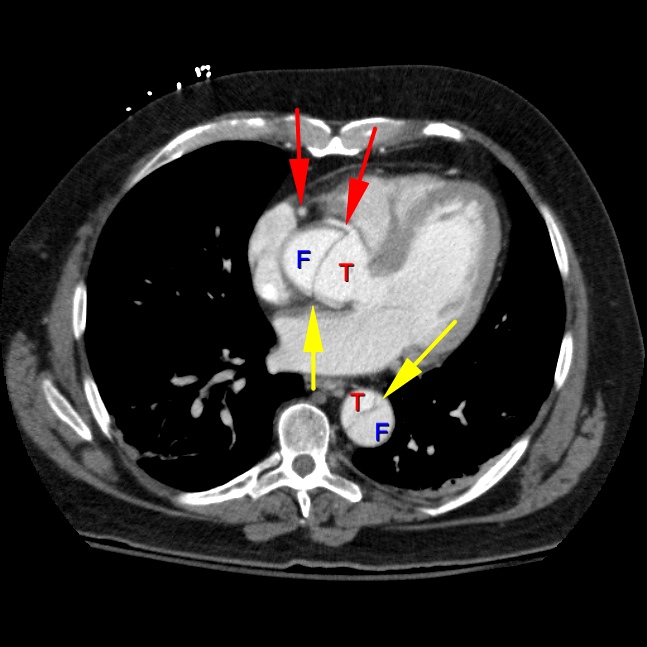
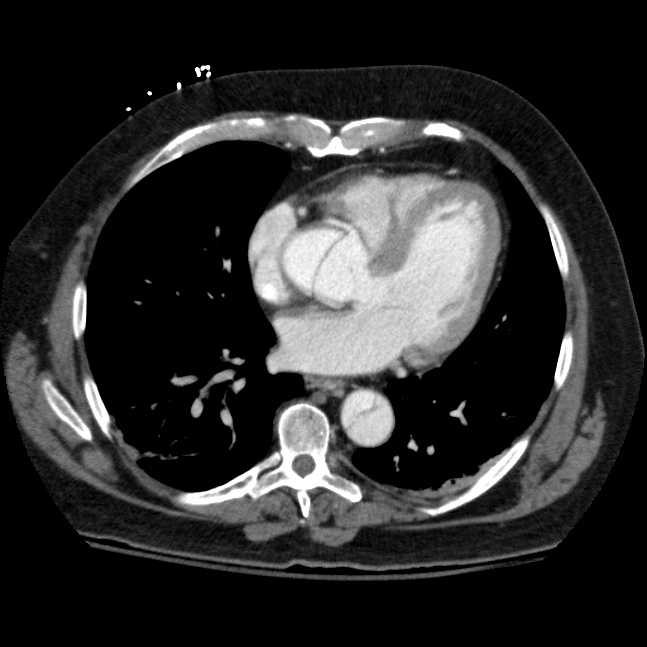
Axial contrast enhanced CT image of the chest at the level of the coronary arteries (red arrows) demonstrates a dissection flap (yellow arrow) with a true lumen (T) and false lumen (F). Since the aortic dissection begins before the left subclavian artery, it is considered a Stanford Type A.
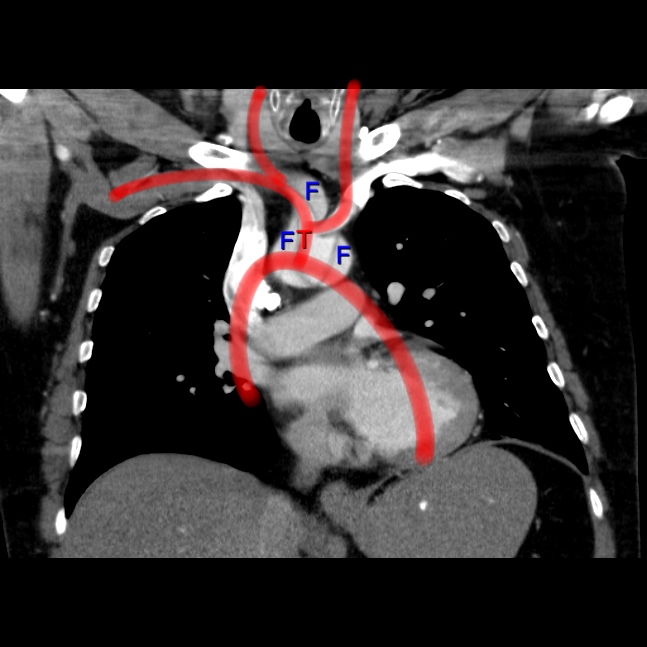
Coronal contrast enhanced CT image of the chest at the level of the aortic arch demonstrates a dissection flap with a true lumen ( T and red highlight) and a false lumen (F). Note the false lumen extending into the brachiocephalic artery. View the next key finding.
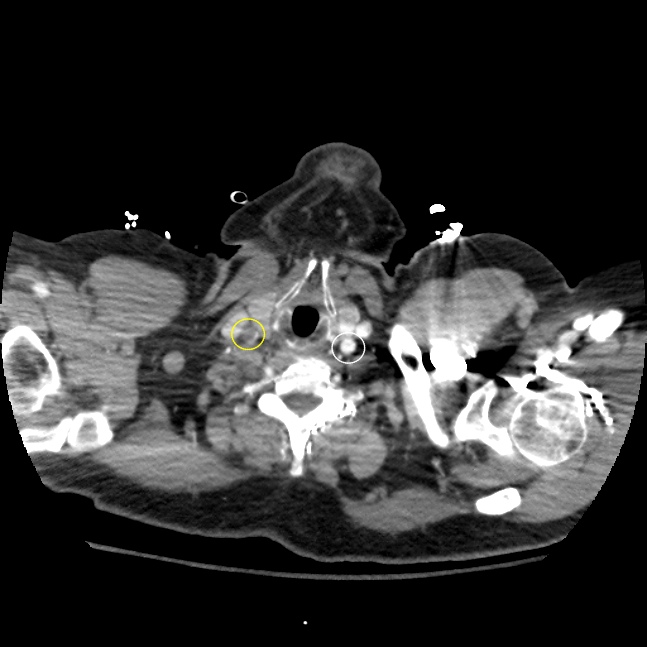
Axial contrast enhanced CT image of the chest at the level of the carotid bulbs. There is near total occlusion of the right common carotid artery (yellow arrow) secondary to the dissection flap. Compare the abnormal right common carotid artery (yellow circle) with the normal left side (white circle). This finding demonstrates a reason why Stanford A type of aortic dissections are surgical emergencies. If the dissection begins distal to the takeoff of the left subclavian artery, it is considered a type B and can be treated more conservatively.